If you've dealt with reflux, joint pain, or both, there's a good chance two types of medication have passed through your hands: a proton pump inhibitor like omeprazole, and an NSAID like ibuprofen or naproxen. They're sold - and often prescribed - as low-risk, everyday solutions. The research tells a more complicated story, and it's one worth understanding before either becomes a long-term habit.
Omeprazole: solving the symptom, not the mechanism
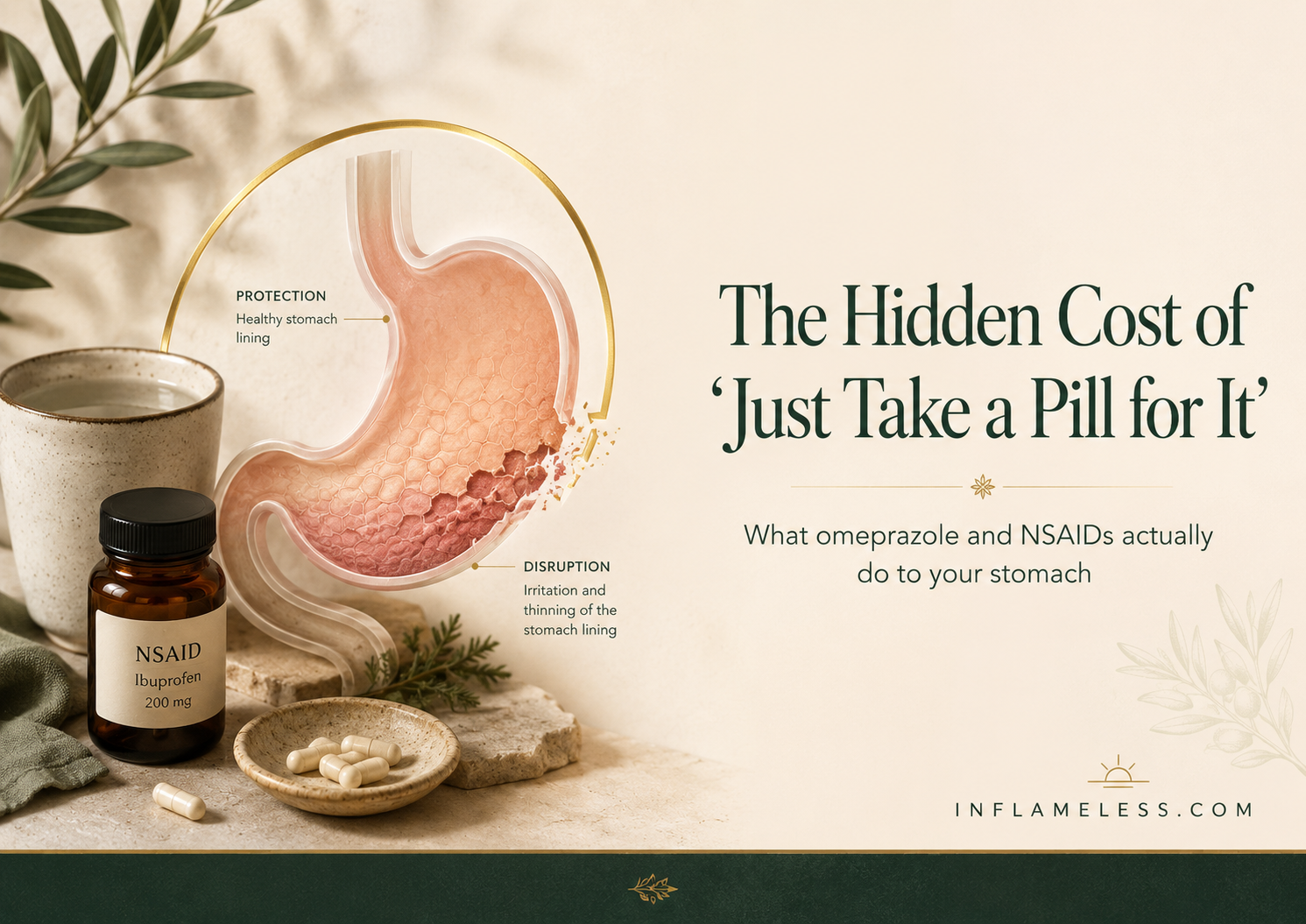
Proton pump inhibitors work by shutting down the acid pumps in your stomach lining. This is precisely why they're so effective at stopping heartburn - if there's dramatically less acid, there's nothing left to reflux upward and burn. But that same acid was never the villain to begin with. Your stomach runs at a strongly acidic pH by design, because that acidity is required to unfold proteins, absorb minerals, and neutralize pathogens arriving with food. Suppressing it doesn't fix a location problem; it just removes the substance that was flagging it.
The clinical literature has been tracking what happens when that acid production stays suppressed for months or years.
Nutrient absorption declines. Stomach acid is required to release vitamin B12 from the proteins that carry it, and to convert dietary iron into a form your body can absorb. Long-term PPI users show measurable declines in B12 status, with one review of older adults on extended PPI therapy finding a 12-18% drop in serum B12 over just twelve months. A separate case-controlled study found that PPI use for two years or more significantly increased the risk of clinically diagnosed B12 deficiency, particularly at higher doses. Calcium and iron absorption follow a similar pattern, since both depend on the same acidic environment to become bioavailable.
Small intestinal bacterial overgrowth becomes more likely. A meta-analysis pooling eleven studies and over 3,000 participants found more than double the risk of SIBO among PPI users compared to non-users - and the association was even stronger in studies using more sensitive detection methods. The mechanism lines up with everything acid is supposed to do: without sufficient stomach acid to act as a barrier, bacteria that should be neutralized before reaching the small intestine survive and colonize it instead.
Stopping isn't simple. This is the part rarely explained at the point of prescription. A randomized, placebo-controlled trial in healthy volunteers - people with no prior digestive complaints - found that eight weeks of PPI therapy induced acid-related symptoms in 40-50% of participants after the medication was withdrawn, symptoms that weren't present before treatment started.[5] The mechanism is called rebound acid hypersecretion: prolonged acid suppression triggers elevated gastrin levels, which in turn drives the growth of acid-producing cells, so that stopping abruptly can leave the stomach producing more acid than it did before treatment ever began.[6] Studies measuring this effect directly show gastrin and acid output can take one to two weeks to normalize after stopping.[7] In practice, this rebound is what convinces many people they can never come off the medication, when what they're often experiencing is a temporary withdrawal effect rather than a return of the original problem.
None of this means PPIs have no place - for a diagnosed ulcer or acute mucosal injury, short-term use is genuinely appropriate. The concern is specifically with indefinite, unsupervised long-term use for reflux that may have a different root cause entirely: a poorly sealing valve rather than an acid surplus.
NSAIDs: a completely different mechanism, similar outcome
Where PPIs suppress acid, NSAIDs damage the stomach through an entirely separate pathway - which matters because it means the two categories of harm can stack rather than substitute for each other.
NSAIDs work by inhibiting an enzyme called cyclooxygenase (COX), which is how they reduce pain and inflammation. The problem is that the same enzyme, specifically the COX-1 form, is also responsible for producing the prostaglandins that maintain your stomach's defenses: mucus production, bicarbonate secretion, and adequate blood flow to the lining.[8] Block the enzyme system-wide, as most NSAIDs do, and you reduce pain signaling in a joint while simultaneously stripping away the stomach's own protective coating.
The scale of this effect is larger than most people assume. Endoscopy studies of long-term NSAID users find ulceration rates ranging from 15% to 40%, and the damage isn't confined to the stomach - as many as 70% of long-term NSAID users show inflammation in the small intestine, with roughly 30% developing erosions or frank ulcers there as well.[9] This occurs alongside reduced neutrophil defenses and impaired healing capacity, meaning existing damage repairs more slowly while new damage accumulates.[10]
There's an important interaction worth naming here: clinical trial data shows that co-prescribing a PPI alongside long-term NSAID use meaningfully reduces ulcer complications compared to NSAIDs alone.[11] This isn't an argument for taking both indefinitely - it's a reminder that the two drug classes are frequently paired specifically because each is causing a distinct kind of harm that the other happens to blunt, not because the combination is inherently safe.
Why this matters more than either fact alone
Looked at side by side, PPIs and NSAIDs represent two different failure modes converging on the same organ. One strips away a defense the stomach needs (acid, used correctly, is protective). The other strips away a different defense the stomach also needs (the mucus and blood flow that prostaglandins maintain). Someone managing both joint pain and reflux long-term, without medical oversight of the combination, is often working against their own digestive system on two fronts at once.
None of this is a call to stop any medication unilaterally - rebound acid hypersecretion is a real, documented risk of abrupt PPI discontinuation, and NSAID-related pain often has no perfect substitute. It's a case for informed conversations with a physician: asking specifically about tapering schedules, lowest effective doses, and whether the underlying reflux or pain driver has actually been identified, rather than defaulting to indefinite use of either drug class.
Medical disclaimer: This article is for educational purposes only and does not constitute medical advice, diagnosis, or treatment. Proton pump inhibitors and NSAIDs are prescription and over-the-counter medications that should only be started, adjusted, or discontinued under the guidance of a qualified healthcare provider. Do not stop or change any medication based on this article. If you experience symptoms such as difficulty swallowing, unintended weight loss, vomiting blood, or black stools, seek medical attention promptly.
References
- Systematic review of long-term PPI use in older adults on polypharmacy, reporting a 12-18% reduction in serum vitamin B12 over 12 months of therapy. PMC.
- Case-controlled study (Kaiser Permanente) finding significantly increased risk of vitamin B12 deficiency with PPI or H2RA use of two years or more, particularly at high doses.
- Evidence-based review of PPI indications, efficacy, harms, and deprescribing, detailing impaired absorption of vitamin B12, magnesium, calcium, and iron under hypochlorhydria. MDPI.
- Meta-analysis of 11 studies (3,134 participants) reporting a significantly increased risk of small intestinal bacterial overgrowth among PPI users (OR 2.28, 95% CI 1.24-4.21). Mayo Clinic Proceedings.
- McColl KE, Gillen D. Proton-pump inhibitor therapy induces acid-related symptoms in healthy volunteers after withdrawal of therapy. Gastroenterology. 2009;137(1):20-22.
- Review of rebound acid hypersecretion mechanisms, describing hypergastrinemia-driven growth of acid-producing enterochromaffin-like cells following PPI discontinuation. PMC.
- Systematic review of rebound acid hypersecretion after PPI therapy, noting gastrin and acid output normalization within approximately 14 days of discontinuation. NCBI Bookshelf (DARE).
- Mechanisms of gastrointestinal damage from NSAIDs, detailing COX-1 inhibition and reduced mucosal prostaglandin levels as the core pathogenic pathway. Gastroenterology.
- Estimates of NSAID-associated gastroduodenal ulcer rates (15-40% in long-term users) and small intestinal injury (up to 70% with inflammation, 30% with erosions or ulcers). Gastroenterology.
- Review of NSAID gastropathy mechanisms, including reduced mucosal blood flow, impaired bicarbonate and mucus secretion, and delayed healing. Gastroenterology.
- Clinical evidence on reduced incidence of NSAID-related ulcer complications when co-administered with proton pump inhibitors or high-dose H2-receptor antagonists. Gastroenterology.
FAQ Section
Can omeprazole cause nutrient deficiencies?
Long-term proton pump inhibitor use may reduce absorption of nutrients that depend on stomach acid, including vitamin B12, iron, calcium, and magnesium.
Do NSAIDs damage the stomach lining?
NSAIDs can reduce protective prostaglandins, which help maintain mucus, bicarbonate, and blood flow in the stomach lining.
Is it safe to take omeprazole and ibuprofen together?
Sometimes doctors prescribe a PPI with NSAIDs to reduce ulcer risk, but this should be medically supervised, especially with long-term use.
Can stopping omeprazole suddenly make reflux worse?
Yes. Some people experience rebound acid hypersecretion after stopping PPIs abruptly, which can temporarily worsen symptoms.
Should I stop taking omeprazole or NSAIDs?
No medication should be stopped or changed without medical guidance. The safest step is to ask your doctor about dose, duration, alternatives, and tapering if needed.

{kind=link}